
Common Objections to Delayed Cord Clamping – What’s The Evidence Say
Many maternity care providers continue to clamp the umbilical cord immediately after an uncomplicated vaginal birth, even though the significant neonatal benefits of delayed cord clamping (usually defined as 2 to 3 minutes after birth) are now well known.
In some cases this continued practice is due to a misunderstanding of placental physiology in the first few minutes after birth. In others, human nature plays a role: We are often reluctant to change the way we were taught to do things, even in the face of clear evidence that contradicts that teaching.
Though there is no strong scientific support for immediate cord clamping (ICC), entrenched medical habits can be glacially slow in changing. Here are some often-heard objections to delayed cord clamping (DCC), and how an advocate for delayed clamping might respond to them:
1) I have a very busy practice. DCC takes too much time!
Not really, especially when you consider the benefits. Nearly one-third of a baby’s total blood volume resides in the placenta at birth. Half of that blood is transfused into the baby by 1 minute of age. By 3 minutes, more than 90% of the transfusion is complete. (1)
2) Immediate clamping helps prevent severe postpartum hemorrhage.
There is no convincing evidence to support this view. Several large studies, including a 2009 Cochrane review of 5 trials involving more than 2,200 women, have found no significant difference between ICC and DCC in terms of postpartum hemorrhage or severe postpartum hemorrhage. (2-6, 10)
3) A healthy, term baby doesn’t get much benefit from delayed clamping.
Though this is a commonly held belief, it’s definitely untrue.
Whether a fetus is premature or full term, approximately one-third of its total blood volume resides in the placenta. This is equal to the volume of blood that will be needed to fully perfuse the fetal lungs, liver, and kidneys at birth.
In addition to the benefits that come with adequate iron stores (see below), babies whose cords are clamped at 2 to 3 minutes – and thus, who have an increased total blood volume compared with their immediately-clamped peers – have a smoother cardiopulmonary transition at birth.
A third benefit: stem cells, which play an essential role in the development of the immune, respiratory, cardiovascular, and central nervous systems, among many other functions. The concentration of stem cells in fetal blood is higher than at any other time of life. ICC leaves nearly one-third of these critical cells in the placenta. (1,3,4,6-10)
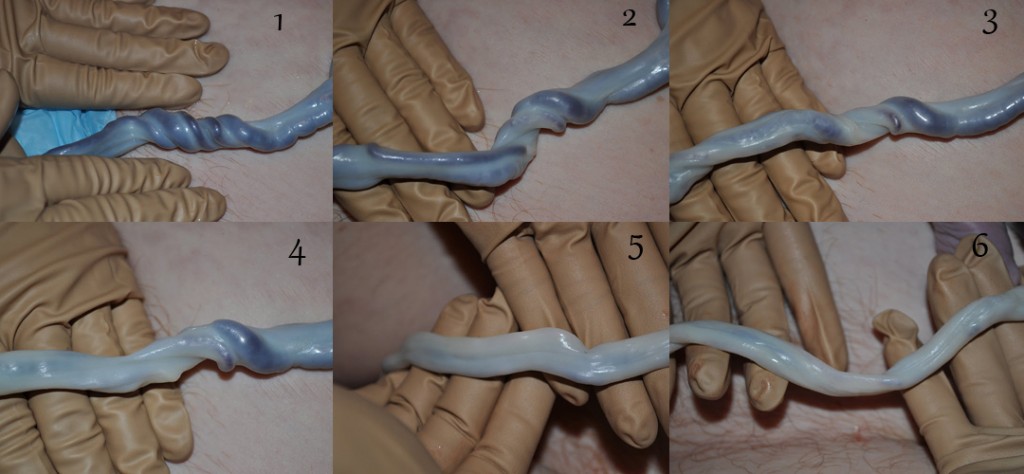
Unclamped cord over the course of 15 minutes.
photo nurturingheartsbirthservices.com
4) Okay, so delayed clamping means a baby gets more blood and more iron. But iron deficiency isn’t really a problem in first-world countries, right?
Wrong. At least 10% of the general U.S. toddler population (1-3 years of age) is iron deficient, with the prevalence rising well above 20% in selected ethnic and socioeconomic populations.
Immediate cord clamping is only one of many factors that contribute to iron deficiency in early childhood. But babies who start out life low on iron have a very difficult time catching up. Delayed cord clamping provides a baby with as much as a 4- to 6-month supply of iron. (1,3,6-10)
5) Doesn’t iron deficiency just make kids tired?
Iron deficiency does much more damage than that. Early infancy is a time of rapid brain growth and development, and iron is essential to that process. Studies of infants with iron deficiency have found specific deficits in cognitive processing (including attention and memory) which may lead to permanently decreased intellectual functioning. Making matters even worse, children with severe iron deficiency often exhibit ’emotional dulling’ – difficulty engaging with caretakers and their environment – which can lead to long-lasting social-emotional deficits. For many reasons, early infancy is a particularly bad time to be low on iron. (1,11)
6) Don’t babies get plenty of iron from breast milk?
Unfortunately, no. While breast milk contains a remarkable array of healthful components, a high concentration of iron isn’t one of them. This most likely has to do with maternal recovery from childbirth. A recuperating mother has her own urgent iron needs; replacing the blood typically lost in childbirth takes a lot of it. Nature intends babies to get most of the iron they’ll need for their early development from the placental blood reservoir, rather than from mother, and so comparatively little iron goes into breast milk. (3,7)
7) But the baby can lose significant blood volume back into the placenta (aka ‘backflow bleeding’) if clamping is delayed.
This is extremely unlikely in an uncomplicated birth. With some brief exceptions (e.g., between uterine contractions, or when a baby bears down during crying), blood flow immediately after birth is primarily one-way, from placenta to baby. Here’s a brief explanation of why this is true:
In a process that begins during labor and accelerates as the newborn begins to cry, the pulmonary blood vessels, which receive very little blood flow during pregnancy, open and fill. This relatively sudden change causes the newborn’s blood pressure to fall below the pressure in the placenta. Placental blood, driven by strong uterine contractions, follows the pressure gradient and flows through the umbilical vein into the baby.
As the newborn’s oxygen saturation increases, the umbilical arteries close, which stops nearly all blood flow from baby to placenta. The umbilical vein, which isn’t sensitive to oxygen, remains open somewhat longer, allowing a final bit of blood to flow from placenta to baby before it, too, closes.
The lack of significant ‘backflow bleeding’ is confirmed by the fact that DCC results in ~ 30% greater neonatal blood volume than does ICC. (1,12)
8) DCC can lead to dangerously high levels of neonatal jaundice.
Since bilirubin, the source of neonatal jaundice, originates in red blood cells, it seems logical that the increased blood volume associated with delayed clamping could lead to severe hyperbilirubinemia.
Yet while some studies have demonstrated mildly increased bilirubin levels in DCC babies in the first few days postpartum, most have found no significant difference between DCC and ICC.
This seeming paradox – relatively stable bilirubin levels in the face of substantially increased blood volume – may have to do with increased blood flow to the neonatal liver that comes with the higher total blood volume associated with DCC. Yes, more blood means more bilirubin, which in turn could mean more jaundice, but better blood flow allows the liver to process bilirubin more efficiently. (3,4,6,7,9,10)
9) Delayed clamping can lead to neonatal hyperviscocity – ‘thick blood’ that can cause kidney damage and strokes.
DCC can lead to a somewhat higher neonatal hematocrit than ICC, which isn’t surprising given the additional blood volume. Yet, despite fears of thicker blood ‘sludging’ in organs like the brain and kidneys, no studies have demonstrated this to be the case from DCC alone. (4,6,9,10)
10) You can’t have both the benefits of DCC and immediate skin-to-skin contact. If you place a newborn on his mother’s abdomen (i.e., above the level of the placenta), gravity will reduce the flow of blood from placenta to baby.
Gravity does matter, but mainly in terms of the speed of the placental transfusion. A baby held below the level of the placenta will receive a full transfusion in about 3 minutes; one held above the placenta (e.g., a baby in immediate skin-to-skin contact) will also receive a full transfusion – it just takes a little longer (about 5 minutes). (1,13)
11) But what if the baby needs resuscitation? Isn’t it best to hand her over to the pediatrician immediately?
One of the first things a truly sick baby in the NICU is going to receive is fluid support – often as a 20 to 40 ml/kg bolus of normal saline or blood. Yet that is exactly what’s left behind in the placenta with ICC – about 30 ml/kg of whole blood. There is considerable evidence that sick babies, both term and preterm, have better outcomes with DCC. It’s better to let nature do its own transfusing. (14-16)
Summary:
Delayed cord clamping promotes a healthy neonatal cardiopulmonary transition, prevents iron deficiency at a critical time in brain development, provides the newborn with a rich supply of stem cells, and helps sick neonates achieve better outcomes – all with little apparent risk to mother or baby. The evidence of benefit from DCC is so compelling that the burden of proof must now lie with those who wish to continue the practice of immediate clamping, rather than with those who prefer – as nature intended – to wait.
Source: Dr. Mark Sloan